
Diabetes is the number 1 killer of women and number 2 killer of men in South Africa (Stats SA). There is no national diabetes education programme (University of Pretoria). People are dying because they do not understand their condition (CDC). Diabetes education in South Africa disallows many people living with diabetes to fully understand and manage their condition, and participate in decisions concerning their own lived experience. The problem we want to solve is diabetes education: in the right format, and the right language, at the right health literacy level, to the right person, exactly when they need it.
Among South Africans with internet access, 96% use WhatsApp, representing 76% of the total population. We can meet people where they are, reaching those who need diabetes education most: easily and sustainably, at no cost to them. Foundational diabetes education delivered through WhatsApp has not been done in South Africa, and we are building a framework to make it easier to scale in other African countries. We are also working with South Africans with diabetes at every stage, ensuring what we are building is truly useful and reduces the risk for premature mortality, unequal treatment and/or misinformation for prevention.
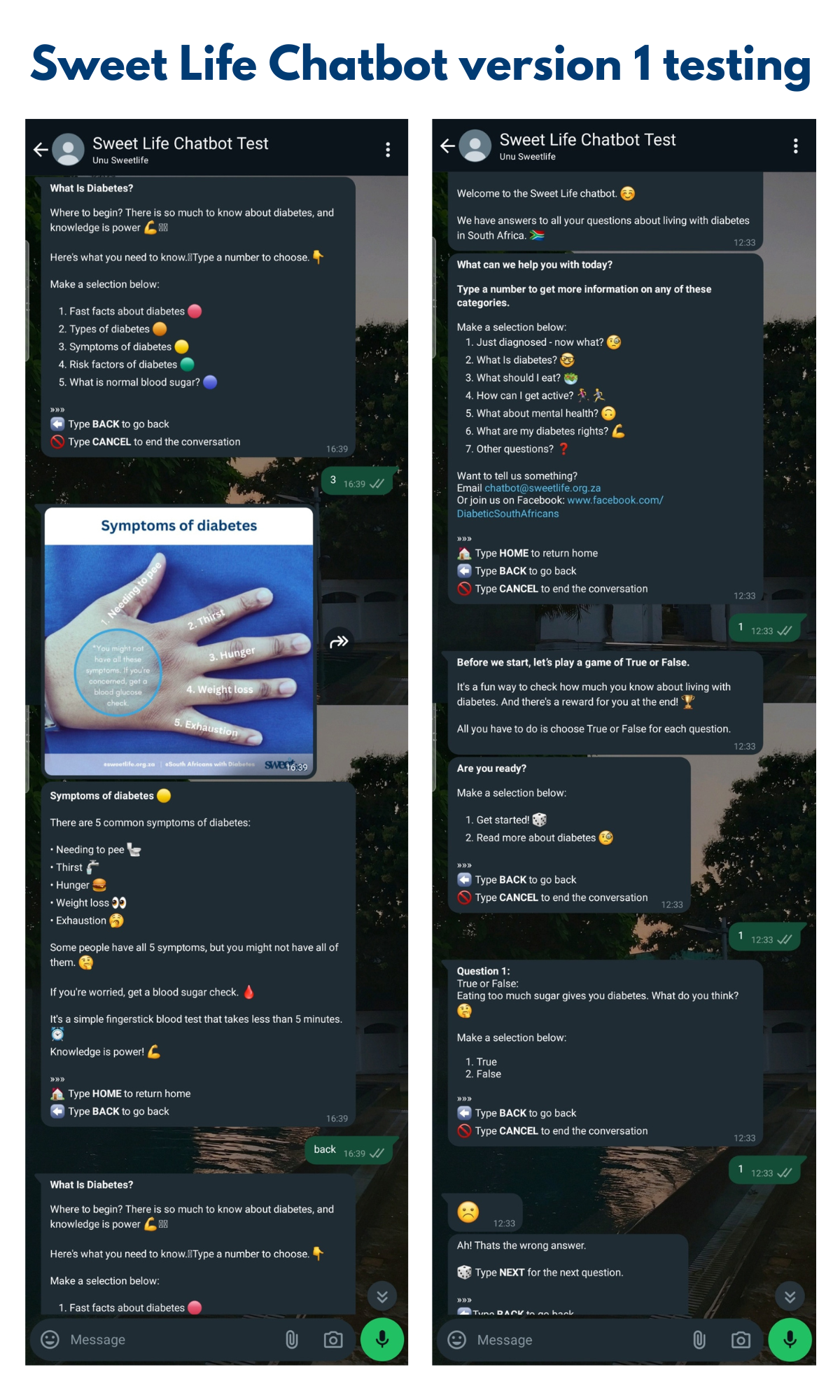
Version 1 of the Sweet Life Chatbot will be released to the public through our launch funder (Unu Health) in July 2024. We have focused this version on six themes: 1. Just diagnosed 2. What is diabetes? 3. What should I eat? 4. How can I get active? 5. What about mental health? 6. What are my diabetes rights? Unu’s national reach will help us get significant users of V1. We then embark on a nationwide feedback drive, accessing outlying diabetes community groups in each province. Refining the tool using feedback evaluation from this drive and our community will result in V2 in early 2025.
Developing foundational diabetes educational tools since 2021 has taught us effective methods to communicate with the general public. Our idea for the 2023 DCB Innovation Challenge became viable when we made it to the Top 3. This momentum led to creating V1 in a very short space of time: initiating a content testing group to launch in both English and isiZulu based on community feedback. A concrete benefit that answers an urgent need for our community is a specifically South African budget meal plan. In addition, the framework we have built can be fairly easily replicated in other African countries.
https://sweetlife.org.za/
This will include the development of a platform that is useful and accessible to South Africans with lived experience of diabetes, and could include helpful referrals to specialist areas such as mental health support. This will not be a primary source of medical advice, but rather support the dissemination of basic information, approved by various reputable sources, for understanding the condition.
2. Empower the existing South African diabetes community through easy-to-understand answers to all their diabetes questions.
We will consistently conduct in-person and virtual feedback engagements to understand the best format and direction of content, so that we can build an understanding of what empowers the South African diabetes community. This can allow for prompted as well as passive channels of communication for the user to provide feedback. This will not assume what topics are important to the community, but rather use the insights of users (people living with diabetes, healthcare teams, caregivers, diabetes organisations) to inform future content updates and refinements.
3. Make it simpler for undiagnosed South Africans with diabetes to find reliable, easy to understand information about diabetes.
This will be achieved through very simple, clear content in the form of informative text, shareable resources and basic quizzes, making it easier to understand the symptoms and basic facts about diabetes. These will be developed for the health literacy of the average South African, which is at Grade 4 to 7 level. This could include referrals to community support groups or further sources of information. The information would not be a medical diagnosis, and it will be made clear that the platform does not replace or supersede the medical advice of healthcare workers.
4. Work with the National Department of Health to use the Sweet Life Chatbot as a national diabetes education programme.
We will seek out opportunities to utilise the tool within government health services to ensure a wider spread of access to the tool, in order to support healthcare workers in accurate information sharing. It should be adaptive to the varying contexts, languages and access of the South African diabetes community. This could aid in alleviating the pressure on clinic staff to prepare a newly diagnosed person with diabetes in the short amount of time generally allocated within the public healthcare space. This would not replace the primary healthcare advice given at clinics, but rather be an accurate source to refer to for the user, enabling them to understand their condition and make better informed decisions on self-management.
All the foundational diabetes educational materials that Sweet Life has developed thus far have been in collaboration with our panel of diabetes experts and endorsed by SEMDSA (the Society for Endocrinology and Metabolism in South Africa). All materials are also submitted to the National Department of Health NCD Department for review, with any feedback incorporated into later versions. We have also worked closely with Dr. Kibachio Joseph Mwangi, the Medical Officer and Advisor for Non Communicable Diseases and Mental Health; World Health Organization (WHO) South Africa, to ensure our diabetes education focus is aligned. In addition, we believe that the power of behavioural change is essential to any education project. We assess any educational materials with behavioural scientist Dr Brendan Maughan-Brown, who has worked extensively in the HIV education space, to ensure that we are looking at education through a behavioural change lens. The strategy for monitoring a project that seeks to impact the quality of life, wellbeing, but also the ease of accessing information to empower individuals and groups requires a mixed methods approach to both quantitatively and qualitatively understand and integrate our offering more effectively. With the project objectives in mind, this will include two main elements that guide our product development: 1) User experience, and 2) Platform refinement. Questions will be framed around the themes detailed below, and provide quantitative data to analyse, with qualitative data collected to gain further insights into the user’s ratings. This will be collected through: - A baseline survey for feedback groups, and as many additional users as possible. - Feedback collected via feedback drive survey and data driven engagement. - Consistent feedback from a group of recurring users, spread throughout the country: this will include agreed upon timelines for collecting feedback, and mobile data to complete the surveys will be provided. - Our network of dieticians, doctors and nurses to complete bi-annual feedback: this will include agreed upon timelines for collecting feedback. - Feedback channel that is available to users, using the email address provided via the chatbot menu. - Consistent feedback through the WhatsApp chatbot platform (to highlight missing information) and through Sweet Life’s online diabetes community. - The option to discuss their experience can also be scheduled within the feedback collection process every six months. 1) User experience, evaluating impact This element explores our understanding of the user; what kind of support they need from a tool like this, what they care about in regards to diabetes care and management, and how the tool can better aid them in meeting these needs. It can also explore how the tool has changed their management and lifestyle, mindset and view of diabetes. Questions will be asked using a rating scale (“On a scale of 1 to 5, how useful did you find the Sweet Life Chatbot?”), with an accompanying prompt to gain insight (“What is your reason for your rating?”). 2) Platform refinement, measuring effectiveness This element explores the value of our offering using the components that make up the platform; the relevance of the content, the usability of the tools and the levels of engagement on the platform. Questions will be asked using a rating scale (“On a scale of 1 to 5, how likely would you be to recommend the Sweet Life Chatbot”), with an accompanying prompt to gain insight (“What is your reason for your rating?”). With consistent questions throughout feedback, we will build the net promoter score (NPS) for the project offering, aiding in not only our understanding of the impact that the tool has on the user’s understanding of diabetes, their ability to make informed decisions about self-management and lifestyle choices, but also measuring the effectiveness of the presentation, navigation and comfortability of the tool. These insights help us assess and improve on the experience of the user with their own suggestions and comments. Further to this, surveys will be as short as possible (5-10 minutes) to reduce potential survey fatigue. Feedback users will be selected using the following list: - Using the engagement facilitated by the feedback drive that will happen during the pilot phase of implementation, an offer to provide further and continuous feedback will be given to the participants. This will help to reach a geographically widespread group to provide feedback. - An offer to provide further and continuous feedback will be given to the pilot group users to track the usefulness of changes. - A similar ratio of people with lived experience of Type 1 and Type 2 diabetes will be included. - Healthcare workers will be included in the feedback groups - Details on the feedback users will be collected to understand any differences or similarities in different contexts. This will be tracked through age, gender, connection to the diabetes community, type of residence (rural, peri-urban, urban), and their expectations.
Sweet Life Chatbot Theory of Change: “If South Africans with diabetes are given diabetes education that they understand, they will be able to manage their condition better, which will ultimately result in less deaths due to diabetes.” In more detail: If South Africans with diabetes are given accessible, relevant information about diabetes management, healthy eating, exercise, mental health and their diabetes rights, in easy-to-understand language and formats, it will increase their awareness and understanding of diabetes. This will increase their confidence in navigating barriers like lack of resources and stigma, so that they can be empowered to effect behavioural changes with regards to medication adherence, healthier eating habits, regular exercise and acceptance and management of their condition. In time, this will lead to reduced hospitalisations, reduced complications, better long-term health and reduced mortality as a result of diabetes in South Africa. This theory guides the initial phases of the project’s implementation, until December 2025. Throughout these phases, the project activities allow us to track and begin to understand the behavioural changes created by this tool. With the conclusion of each phase a project report will be collated, to enhance a culture of adaptive awareness and learning so that we can reflect on success, challenges and lessons learned as a project team.
This project follows a mixed method approach to monitoring project activities and evaluating the project's overall impact. We want to ensure that we are able to gain statistical insights into the usefulness of the chatbot, but also to understand the user experience in order to improve the tool. In addition to this, the process of content maintenance and updates will be directed by the user experience, as well as the best practices we form. To ensure consistent feedback, we will form a group of users that will use the chatbot and provide consistent feedback at scheduled project intervals. Overall project goal: Diabetes education: in the right format, and the right language, at the right health literacy level, to the right person, exactly when they need it. 1) Understanding the user: - Baseline survey for user feedback group to build a reference point for measuring change. This will be carried out through engagements during the feedback drive during the project’s pilot phase. - Data will be collected at six month intervals, using a mixed method approach. Quantitative data will be continuously collected through the platform’s back-end and analysed every six months to monitor progress - this will include: i) How many people are using the chatbot? ii) Number of recurring users iii) Number of complete/incomplete journeys iv) Number of one time users Qualitative data will be continuously collected through the platform’s back-end and analysed every six months to monitor progress - this will be collected from the platform’s open ended feedback channel, as well as from the feedback sent to the email address provided within the chatbot - Every six months, data will be collated through scheduled feedback engagements with recurring user groups and analysed with a mixed method approach. This will build on the baseline survey to help us understand specific elements of the chatbot such as the effectiveness of the content in terms of self-management, empowerment of the user to confidently make decisions, gaps in the knowledge base and understanding why a user does or does not return to the tool. 2) Refining the tool: - Every six months, data will be collated through scheduled feedback engagements with recurring user groups and the platform feedback channels, and analysed with a mixed method approach. Quantitative and qualitative data will be continuously collected through scheduled feedback engagements (surveys, open-ended questionnaires) and the platform’s back-end, and analysed every six months to monitor progress - this will include usage statistics and recurring, complete and incomplete journeys. - Every six months, the team will document learnings, updates and analysed data in a project report. This will function as a reporting tool, as well as a report of learnings that support decision making in the project journey, available to funders, partners and stakeholders, and beneficiaries. This will include a team report on: i) Analysis of the data collected to assess progress towards project goals ii) Findings in the context of project objectives and external factors iii) Successes for the reporting period iv) Challenges for the reporting period v) Learnings for the reporting period vi) Next steps for the project implementation Over and above the overall project goal monitoring, the following monitoring and evaluation for specific objectives will occur: - Objective 1: Centralise reliable basic diabetes information in a widely accessible format for South Africans. Every six months, the following data will be collated through scheduled feedback engagements with recurring user groups and analysed qualitatively and quantitatively: i) Has the right information been centralised? ii) Are there any content gaps? iii) What do we need more information on? iv) Does content resonate with groups - and how to inform and improve from here (What are the reasons that users do not return to the tool? What are the reasons that users do return to the tool?) This will be achieved using a survey that includes a rating scale, as well as prompts for more detailed responses. - Objective 2: Empower the existing South African diabetes community through easy-to-understand answers to all their diabetes questions. Every six months, the following qualitative data will be collated through scheduled feedback engagements with recurring user groups and analysed: i) Do people feel empowered by a centralised source of basic diabetes information? ii) What elements help them feel informed? iii) How has this tool empowered them? - Objective 3: Make it simpler for undiagnosed South Africans with diabetes to find reliable, easy-to-understand information about diabetes. i) Collate how many people are accessing the Healthy Lifestyle sections (food, exercise, mental health) of the chatbot. ii) See if there is any transition from these sections to the purely Diabetes sections of the chatbot. iii) Track how many new users are coming to the chatbot – this speaks to it becoming a useful tool for South Africans to find reliable information about diabetes. - Objective 4: Work with the National Department of Health to use the Sweet Life Chatbot as a national diabetes education programme. Every 6 months, a progress report will be generated to assess whether the chatbot is effective. As part of the issue, a gap identified is the lack of a national diabetes education programme. We can monitor the progress of achieving this objective through including in the biannual report: i) The number of meetings held with the National Department of Health (quantitative). ii) Feedback on developments within meetings with the National Department of Health (qualitative). iii) Future planning with the National Department of Health to integrate the chatbot as a tool to support integrated health care (qualitative).
Phase 1 (February - July 2024) - Content, collation development & formatting (Feb - April 2024) - Monitoring and Evaluation framework development (Feb - June 2024) - Document decisions, plan for future activities (Feb - June 2024) - Platform development and testing with development partner (April - July 2024) Milestone 1: Sweet Life Chatbot version 1 released (July 2024) Phase 2 (August 2024 - January 2025) - Bi-Annual Progress Report 1 initiated (1 August 2024) - Feedback drive to collect and integrate user insights into next version (date to be confirmed based on funding) Milestone 2: Bi-Annual Progress Report 1 completed (30 August 2025) Milestone 3: Feedback drive completed and feedback collated (October 2024) - Refresh of project framework - a review of where we’re at and where we’re headed (October 2024) - Version 2 planning (November 2024) - Version 2 development (December 2024) - Bi-Annual Progress Report 2 initiated (January 2025) Phase 3 (February - July 2025) - Chatbot update platform integration (February/ March 2025) Milestone 4: Bi-Annual Progress Report 2 completed (February 2025) Milestone 5: Sweet Life Chatbot version 2 released (March 2025) - Refresh of project framework - a review of where we’re at and where we’re headed (May/June 2025) Phase 4 (August - December 2025) - Version 3 planning (August 2025) - Version 3 development (August - October 2025) - Bi-Annual Progress Report 3 initiated (November 2024) Milestone 6: Bi-Annual Progress Report 3 completed (December 2025) Milestone 7: SweetLife Chatbot Version 3 released (December 2025)
- High risks (likely to occur with significant/critical impacts): 1. Misunderstanding of advice given, leading to poor lifestyle choices: We have made the language and health literacy of the chatbot very simple, and have assessed it with our feedback group. We also specifically made the food advice in photographic form to eliminate misunderstandings. - Medium risks (possibly will occur with moderate consequences): 2. Backend of platform crashes: None of the information that we share is critical to survival, so if the platform crashes it will be frustrating but will in no way harm the individual using the chatbot. 3. Healthcare workers outside of existing network are not supportive: We understand that the introduction of new tools can be frustrating for a busy healthcare worker. Our integrated approach does not rely on one source of distribution. We also have integrated dialogues with as many healthcare workers as possible into our project plan, to ensure that we are building a tool that is useful to as many users as possible. 4. No institutional support from the National Department of Health: Related to the above risk, the tool would serve its target audience best with the support of those that distribute basic information to people living with, or supporting those living with, diabetes. Our approach sees the National Department of Health as a potential partner to scaling the chatbot to where it is most needed. Lack of support would mean that the project would potentially need further development to fill any gaps identified by feedback from the National Department of Health, and adjusting the approach to target additional partners. 5. Funding ends before a final version is complete: The current version of the chatbot, although not the complete version, is a useful tool in itself, and can be used by someone that needs it without having continuous updates. Alongside the iterative nature of the chatbot development process is its ability to be useful, reputable and engaging at any point of its development. While we are building it to be truly integrated within the national approach to diabetes management, it has the ability to stand on its own. - Low risks (unlikely to occur with minimal/ negligible impact): 6. Incorrect advice given to user: We have chosen a rigid chatbot structure (based on questions with answers) rather than allowing for free questions, specifically so that no incorrect advice can be given. The user is constrained by the question options and cannot ask for further information because we want to proceed with an abundance of caution. Similarly, we will not be using AI in the near future because of the risk of misinformation. 7. Users taking advice from the Sweet Life Chatbot as their primary healthcare advice leading to a health crisis: The chatbot does not give any specific medical advice, particularly about medication, and will include a disclaimer to seek professional medical advice in the event of emergency medical treatment.
We have kept the budget as lean as possible so that we can operate as a start-up and reach as many people as possible. Our launch costs have been covered, as well as the first 6 months of WhatsApp hosting, and we are now looking for long-term partners who can sustainably fund the chatbot, with bi-annual improvements based on community feedback. South Africa is a relatively inexpensive country in which to work, as the rand dollar exchange rate is very much in the dollar’s favour. In addition, we have a remote working environment that means we do not have any office overheads, and we are a Public Benefit Organisation, which means we do not have to pay any tax (South Africa awards this to non-profit organisations whose work contributes to the public good). This project has the potential to reach millions of South Africans - with and without diabetes. The healthy living advice in the chatbot (food, exercise and mental health) can be applied to all NCDs and, in fact, to all South Africans. The diabetes information is specific to those who have already been diagnosed. Because WhatsApp has such high penetration in South Africa, and because there is such a dearth of cohesive diabetes education, we believe this solution could reach hundreds of thousands of South Africans. Our model remains cost-effective into the future, as hosting and development costs remain consistent, and we would simply have to collate feedback and reiterate content based on that feedback. Content costs may increase if video is the predominant content medium chosen by our community, but we have existing videographers that we have used in the past, and a network of South Africans with diabetes who would like to share their lived experience on video for a fee, rather than using expensive models. We have a 13 year history of creating quality content affordably, and we will approach this project as we do all our projects: as simply as possible for maximum effect and impact.
1. Sweet Life Chatbot concept note: https://drive.google.com/file/d/15cHaRg_6DoEIDLqhzyWJMHxtSPLtk-mC/view?usp=drive_link 2. Sweet Life Chatbot Project Tracker: 3. Budget summary: https://docs.google.com/spreadsheets/d/18BZx7GUa-WztkaCFs1JkCh7UodFyE_o8/edit?usp=sharing&ouid=111498304191481710576&rtpof=true&sd=true 4. Proposal overview: https://drive.google.com/file/d/1xPZ_sbroEQX4F3SboQCmEN9uvLJtMoAo/view?usp=drive_link
www.facebook.com/DiabeticSouthAfricans
{kind=link}
{kind=link}
{kind=link}
{kind=link}